
When symptoms like irregular periods, hot flashes, or sleep changes start showing up, it’s natural to want clear answers — and for many women, that means asking for a hormone test. After all, seeing a number on a lab report feels like proof that something real is happening.
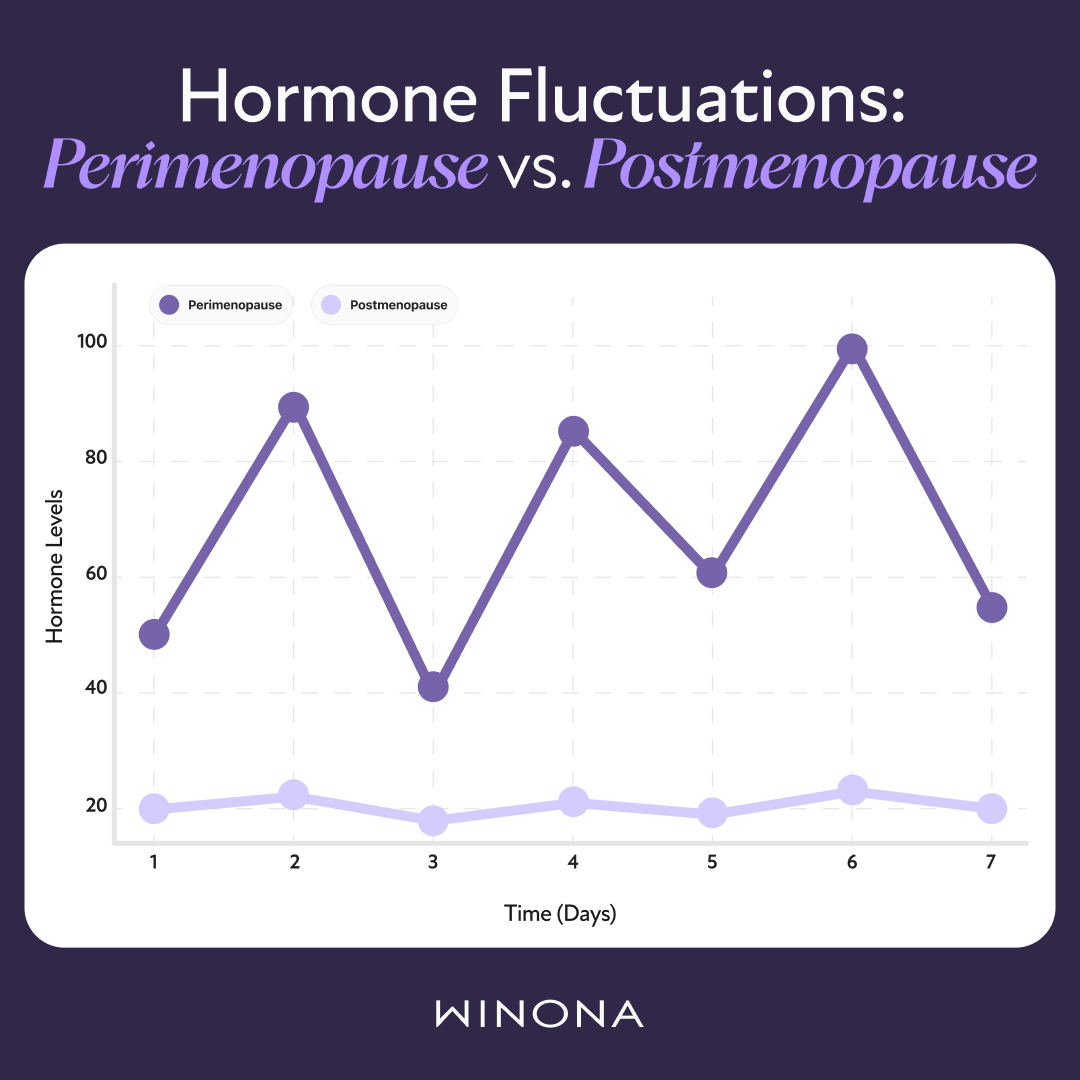
Blood tests for hormones like follicle-stimulating hormone (FSH), luteinizing hormone (LH), and estradiol (E2) are often ordered to “check for menopause.” But as helpful as that sounds, these results can be tricky to interpret — especially during perimenopause, when hormones can rise and fall daily.
This guide explains what hormone tests measure, why the results can be misleading, and how symptoms often tell a more complete story.(1)
What you’ll learn:
What the most common menopause-related hormone tests actually measure
Why a test can’t always give clear answers
How doctors really diagnose perimenopause and menopause
What hormone tests are used to check for menopause?
Several hormones play key roles during the menopause transition. While blood tests can measure them, understanding what these numbers mean — and what they don’t — is important.
During menopause, hormone levels shift as the ovaries slowly stop responding to signals from the brain. Estradiol — the main form of estrogen — begins to drop. In turn, the body releases more FSH and LH to try to encourage the ovaries to produce estrogen. These changes are why some clinicians order tests, even though the results can vary day to day.(1)(2)(3)
Follicle-Stimulating Hormone (FSH)
FSH helps the ovaries mature eggs and produce estrogen. As ovarian function declines, the body compensates by making more FSH. Elevated levels (typically above 30 mIU/mL) may suggest that the ovaries are slowing down.(2)
However, FSH levels can fluctuate widely from day to day during perimenopause. One test may show a value in the “menopausal” range, and the next test might not. According to the American College of Obstetricians and Gynecologists (ACOG), this variability makes FSH testing unreliable as a single diagnostic tool for menopause.(4)(5)
Luteinizing Hormone (LH)
LH works closely with FSH to regulate ovulation. During menopause, LH levels often rise, but like FSH, they vary significantly throughout the cycle. LH testing rarely provides a clear picture and is not typically used by clinicians to diagnose menopause.
Estradiol (E2)
Estradiol is the strongest form of estrogen and supports bone health, mood, and overall hormonal balance. During menopause, estradiol levels decline as the ovaries produce less estrogen. Levels below 50 pg/mL are generally consistent with menopause.(6)
Still, estradiol can fluctuate dramatically in the 10 years before menopause onset — one test might look “normal” even if symptoms suggest otherwise. And hormone tests are usually invalid for women on hormonal birth control or certain hormone therapies.
Progesterone
Progesterone supports regular menstrual cycles and helps balance the effects of estrogen. As ovulation becomes irregular, progesterone levels drop. Testing may confirm whether ovulation is still occurring, but it does not determine menopausal status.
Thyroid-Stimulating Hormone (TSH)
Because thyroid disorders can mimic menopause symptoms — including fatigue, mood changes, and irregular cycles — doctors may include a TSH test to rule out thyroid dysfunction.
Hormone | Primary Role | What Happens During Menopause |
FSH | Stimulates egg growth and estrogen production | Rises as ovaries become less responsive |
LH | Triggers ovulation | Rises but fluctuates widely |
Estradiol (E2) | Main form of estrogen | Gradually decreases |
Progesterone | Regulates cycles and supports uterine health | Declines as ovulation stops |
TSH | Controls thyroid hormone production | Usually tested to rule out thyroid disorders |
Major medical bodies like the ACOG and The Menopause Society note that hormone fluctuations make it difficult to draw firm conclusions from a single test — and that diagnosis should rely on clinical history and symptoms rather than lab values.(7)Along with blood tests, two other methods for hormone testing are often marketed to women around menopausal age.
Urine Tests
The DUTCH test (dried urine test for comprehensive hormones) measures hormone byproducts, or metabolites, in urine. The idea is that once hormones complete their work, they are broken down by the liver and kidneys before leaving the body through urine.(8)
However, research has not shown that the DUTCH test helps to diagnose, guide treatment, or manage menopause symptoms. It’s not recommended by medical societies, and its advisory board does not currently include menopause specialists.(7)
The test is also expensive — typically around $600 — and has not been proven to offer more useful information than symptom assessment or standard hormone testing. For any woman considering this test, it’s best to discuss its value and necessity with a qualified menopause healthcare provider before proceeding.
Saliva Tests
Saliva tests were developed as an easy, at-home way to measure hormone levels. They use a method called ELISA to detect hormones in saliva. While convenient, studies show that hormone levels in saliva don’t reliably match blood levels.(7)
Because of this inconsistency, saliva testing is not considered accurate for diagnosing or monitoring menopause or guiding hormone therapy.
Why Test Results Can Be Misleading During Perimenopause
Testing hormones during perimenopause is like taking a single photo on a roller coaster and trying to understand the whole ride. Hormones shift constantly — sometimes even within hours — making test results more of a snapshot than a full story.
A “normal” result doesn’t necessarily mean nothing is changing, just as a “menopausal” reading doesn’t mean the transition is complete. Hormone levels can fluctuate for several years before menopause actually occurs.(7)
Research with the British Menopause Society explains that for women over 45, menopause is better diagnosed based on symptoms rather than blood tests. Blood tests are more useful in specific cases — for example, in women who’ve had a hysterectomy (and no longer have periods) or in younger women under 40 where premature ovarian insufficiency or early menopause is suspected. In these cases, testing can help rule out thyroid problems, metabolic issues, or vitamin deficiencies that cause similar symptoms.(5)(9)
In most cases, however, test results add confusion rather than clarity. FSH might be high one month and normal the next. Estradiol could appear normal even as hot flashes and night sweats intensify. A single test cannot reliably show where someone is in the menopausal transition.(1)
This variability is why most menopause specialists focus on what symptoms reveal — because they reflect how hormones are acting in the body over time, not just at one moment.
Many women share the experience of seeking answers from lab tests but only finding real progress once care focuses on symptoms.
The Gold Standard: A Symptom-Based Menopause Diagnosis
A menopause diagnosis is ultimately based on a clinical evaluation, not a lab result. Physicians consider a combination of factors, including the following:(9)
Menstrual history (how cycles have changed)
Symptom type, frequency, and severity
Overall health, medical history, and lifestyle factors
Many experts recommend keeping a daily or weekly symptom log to share during appointments.
Tracking symptoms — from sleep patterns to mood and menstrual changes — helps reveal patterns that blood work alone can’t show. Keeping a simple calendar or symptom log makes it easier to notice changes over time. Some women also use symptom score sheets to track how severe their symptoms are and to see how well treatments are working.

Numbers can be helpful, but what truly matters is how a woman feels day to day. Listening to her symptoms gives us a more complete understanding of where she is in the transition.
This symptom-first approach enables women to partner with their doctors for personalized care. It moves the focus from “What do my numbers say?” to “What is my body trying to tell me?” — which ultimately leads to more effective treatment decisions.
Finding Clarity Beyond the Numbers
It’s completely understandable to want proof via a test result that explains what’s happening. But when it comes to menopause, hormones rarely follow a straight line. A single test can’t always provide the full picture, and that’s okay.
Clarity comes from understanding both the science and the symptoms. The Menopause Society suggests that working with a physician trained in menopause care ensures every aspect — physical, emotional, and hormonal — is considered.(10)
Experiencing menopausal symptoms? Discover if HRT is right for you.
If symptoms are disrupting daily life, help is available.
Start your visit — Connect with a licensed menopause specialist.
Take the quiz — Get a clearer sense of where you are in the transition.
Hormone levels may fluctuate, but relief and clarity don’t have to.

